A Strengthening Band
Education-Information-Support
Frequently Asked Questions
The University Of Chicago’s FAQ on Cervical Insufficiency.
http://www.uchospitals.edu/specialties/obgyn/cerclage/faq.html
What is Cervical Insufficiency?
Sometime around the second trimester, pressure from the growing fetus may cause the cervix to open prematurely. This condition is called Cervical Insufficiency (or Incompetent Cervix), and may lead to miscarriage or premature delivery.
How often does Cervical Insufficiency occur?
Cervical Insufficiency occurs in only about 1-2% of pregnancies. Nearly 25% of babies miscarried in the second trimester are caused by CI.
What Causes Cervical Insufficiency?
Previous surgery on the cervix
Damage during a previous difficult birth
Previous trauma due to D&C from a termination or a miscarriage
Congenital malformed cervix or uterus
DES (Diethylstilbestrol) exposure
What is the treatment for a weakened cervix?
A procedure which sews the cervix closed to reinforce the weak cervix in an attempt to keep the baby in the womb. This procedure is called a “cerclage” and usually performed sometime after the first trimester. The most common type of cerclage is called a “Transvaginal Cerclage” which is a suture which is placed through the vagina, within and around the cervix, much like a “purse string”.
Why Transabdominal Cerclage (TAC)?
In general, a vaginal cerclage can only be placed so highly on the cervix due to the nature of placement. The higher the placement of the suture or stitch, the more cervical length is preserved. This is important because the length of the cervix protects the amniotic sac and fetus from infection and opening prematurely, causing miscarriage.
The TAC is placed via an incision in the lower abdomen (much like a c-section or bikini incision) or laparoscopically and is approached from the upper portion of the lower uterine segment as opposed to via vaginal route. This allows for the cerclage to be put as highly as possible (at the uterine/cervical junction), reducing the chances for “funneling” or opening of the cervix from the inside. Additionally, due being placed intra-abdominally, there is less risk of infection as there is no suture material exposed to vaginal flora. This eliminates the possibility of “wicking” of potentially harmful bacteria.
Transabdominal Cerclage has traditionally been reserved for:
1) women do not have enough cervical tissue with which to place the standard Transvaginal Cerclage and/or
2) women who have had the Transvaginal Cerclage fail in spite of having it placed prophylactically (prior to any cervical changes).
Transvaginal Cerclages generally hold a 70-80% rate of success VS. Transabdominal Cerclage which holds a much higher rate of success, 90+%. Consider the fact that this high rate of success is among patients who have true Cervical Insufficiency and the 90% success rate becomes even more impressive.
Not every physician performs TAC, yet there are doctors who are specially trained in the procedure and their patients have extremely positive outcomes due to the fact that they are in the hands of skilled and knowledgeable surgeons. Not every patient with Cervical Insufficiency may require a TAC, but if you fall into one or both of the categories listed above, then a TAC may be a viable option.
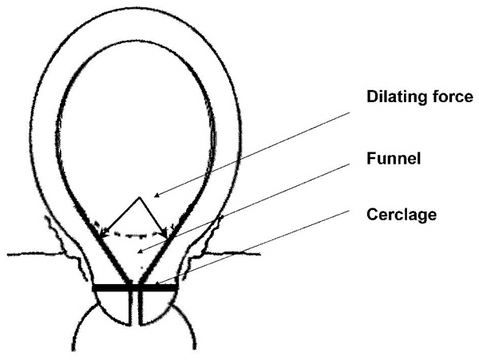
Figure below. The first stage of dilation, funneling, due to the weight of baby, placenta, and amniotic fluid. Note the position of a standard, transvaginal cerclage. The funnel can easily continue to efface and/or dilate the cervix, compromising it’s functionality in being a barrier to bacteria, preventing PPROM and ultimately, preterm labor and early perinatal loss (usually around 16-24 weeks on average).
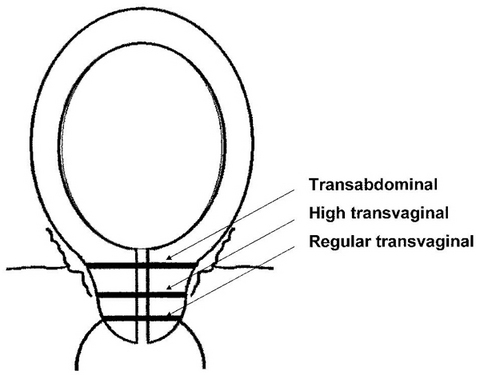
The diagram below clearly demonstrates the level of sutures placed in the cervix in order to prevent perinatal loss due to the condition of Cervical Insufficiency. In general, the lower the suture is placed on the cervix, the greater chance for funneling of the amniotic sac, increasing the chances of dilation and/or infection and ultimately, second trimester loss of a non-viable fetus.
In the case of a high transvaginal cerclage, there is space for funneling.
The transabdominal cerclage (TAC) is placed at the uterine/cervical junction, as high on the lower uterine segment as possible. This tremendously decreases the chance of funneling as there is essentially no cervix above the TAC, only the amnion. The absence of funneling means that the process of loss due to cervical insufficiency is halted at the initial stage.